UVA Health Among First in Virginia to Use New Stent for Acute Aortic Dissections
Distal malperfusion (lack of enough oxygenated blood downstream from an aortic injury) is one of the most dangerous complications of acute Type A aortic dissection. A successful repair of the ascending aorta doesn't always fix it. Patients can leave the OR with weakened flow to the visceral vessels, renal arteries, and iliac beds, facing a possible second round of procedures on top of an already difficult recovery.
UVA Health was among the first centers in Virginia to use the AMDS (Ascyrus Medical Dissection Stent) device to tackle this problem during the primary repair. John A. Kern, MD, chief of cardiothoracic surgery at UVA Health, calls the new stent and procedure, "a game changer for patients with dissections."
“It goes a long way to treat the malperfusion,” says Kern. “It reestablishes true lumen blood flow and patency. And it does so in a way that actually facilitates the dissection repair. The AMDS device essentially stents open the arch and the descending aorta without the need to perform a complete total arch reconstruction. So, it really makes the operation easier. It makes it shorter.”
The Clinical Problem in Type A Dissection
In an acute Type A dissection, a tear in the wall of the aorta allows for a false lumen to form. Pressure from blood flow in the false lumen compresses the true lumen. This can greatly reduce blood flow to the visceral arteries, renal arteries, and iliac vessels. Repairing the ascending aorta does not always restore true lumen patency further down the artery.
"Even though historically we go in and take care of the ascending aorta, fixing that does not always immediately alleviate distal malperfusion," reminds Kern.
Before the AMDS device, patients with malperfusion after repair needed further intervention. That meant more stenting, surgical bypasses, or both, adding risk and recovery time to an already critical situation.
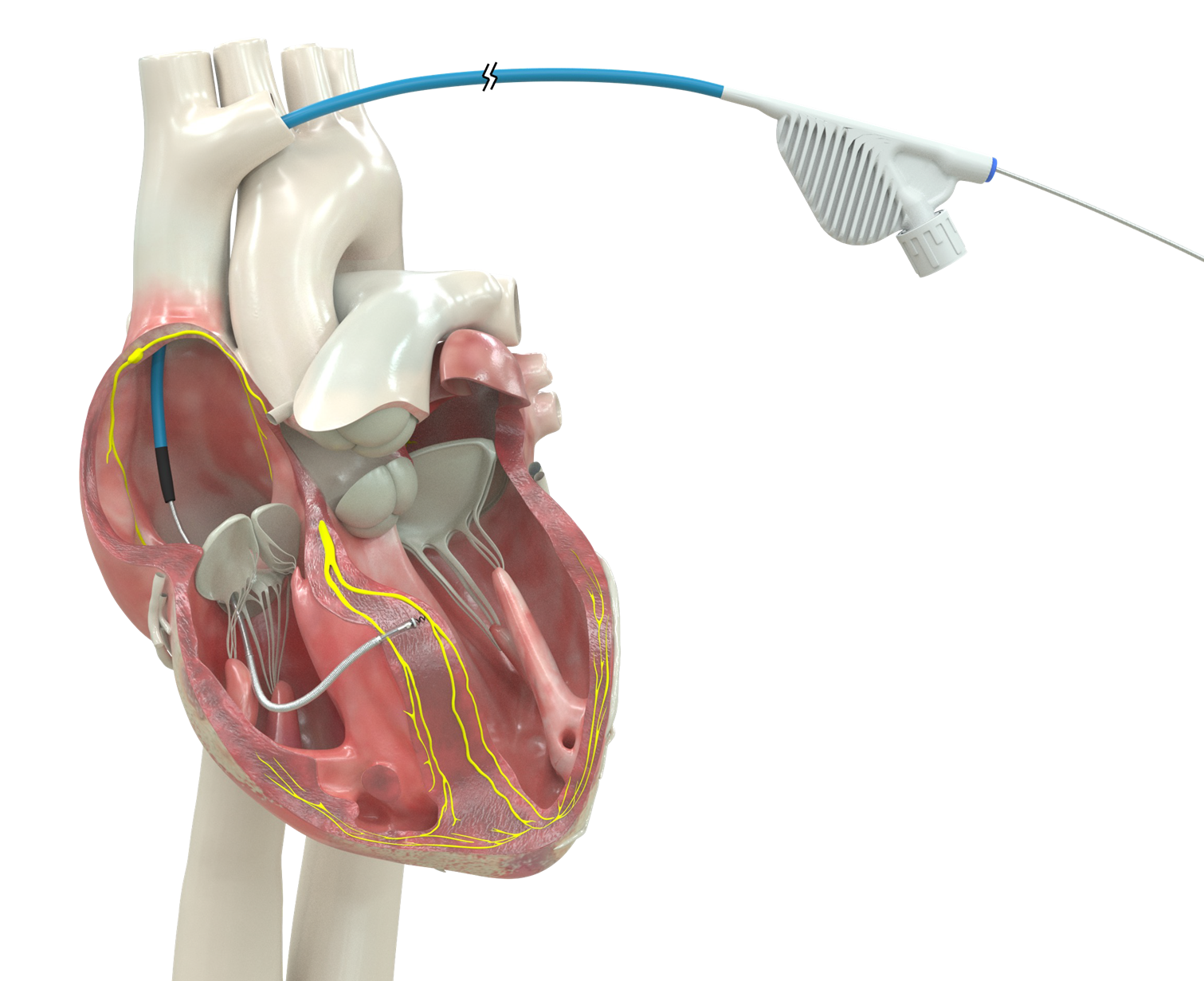
How the AMDS Device Works
The AMDS is a bare-metal, uncovered stent. When deployed, it spans from the aortic arch down into the descending thoracic aorta. That length is what makes it effective.
By stenting open the true lumen across the arch and into the descending aorta, true lumen patency is restored, not just at the level of the stent, but often through the abdominal aorta and into the visceral and iliac vessels.
"This device stents open the true lumen — not just where the stent is, but, because it helps depressurize the false lumen, that true lumen patency is maintained all the way down through the abdominal aorta to the visceral vessels and the iliac arteries," explains Kern.
He credits two features for its performance: "the length and the radial force" (how firmly the stent holds the vessel open against false lumen pressure).
Integrating Into Surgery
The AMDS fits cleanly into the standard repair. Bypass time isn’t extended. "It doesn't change our operation a whole lot at all. It's just an added component to what we already do," notes Kern.
The device also reduces the need for total arch reconstruction in patients without a past arch aneurysm or intimal tear in the arch. It achieves much of the same downstream benefit (arch and descending aorta support, true lumen patency) without the added operative steps. "This actually facilitates the operation a little bit and seems to be very effective," he adds.
Patient Selection & Outcomes So Far
The AMDS works best for patients with acute Type A dissection, distal malperfusion, and a normal-caliber arch and descending aorta.
It is generally not a good fit for patients in two groups:
- Patients with a pre-existing arch aneurysm who already need total arch replacement
- Patients with dissection extending into the great vessels or carotids, where anatomy is more complex
"If you have a normal-sized descending aorta and arch, then I think the AMDS device is really good for those folks with malperfusion," says Kern.
All four patients treated with the AMDS device at UVA Health presented with severe malperfusion. In all four cases, malperfusion resolved after the repair. None required more stenting afterward or open bypass procedures.
In one case, a patient arrived experiencing profound malperfusion, with absent left femoral pulse and reduced perfusion to the abdominal organs and kidneys. After repair with the AMDS device, normal flow was restored to the abdominal aorta and vasculature and lower extremities. He has ongoing renal issues from prolonged preoperative renal ischemia. But he avoided the need for a femoral-femoral bypass and abdominal aortic and visceral vessel stenting that would historically have followed.
"Not only does it correct a bad problem at the time of surgery, but it can also prevent further problems down the road," Kern says. The AMDS is currently available under a Humanitarian Device Exemption, with full FDA approval anticipated.
UVA Health's Aortic Expertise
"We became involved simply because of the large amount of aortic work we do, the large number of dissections we see, and our familiarity with other endovascular devices and stents for dissections," says Kern, reflecting on the depth of our aortic program and our experience with complex dissection repair.
For patients with suspected or confirmed acute aortic emergencies, UVA Health also offers an Aortic Alert System. This standardized, time-sensitive activation process is designed to get patients the care they need as soon as possible.