UVA Health Among First to Perform MRI-Guided Cardiac Ablation

UVA Health is just the second institution in the U.S. to perform a magnetic resonance imaging (MRI)-guided cardiac ablation procedure‚ a major step forward in how we treat arrhythmias.
The procedures were done as part of the VISABL-AFL clinical trial, which tested a new catheter and mapping system and focused on treating typical atrial flutter.
Kenneth Bilchick, MD, MS, a professor of cardiovascular medicine and heart rhythm disorder specialist, led the effort at UVA Health. Three procedures have been performed here, with a fourth scheduled. "People have been working on MRI-guided procedures and ablations for well over a decade,” notes Bilchick. “It’s called iMR, or interventional magnetic resonance, because the procedure is performed directly within the MRI scanner rather than in a standard electrophysiology lab. A major advantage is the ability to directly visualize cardiac structures and ablation delivery in real time. In other words, operators can see the catheter moving within the heart without reliance on X-ray fluoroscopy.”
A New Kind of EP Lab
Standard electrophysiology (EP) procedures use fluoroscopy to guide catheter placement. That means radiation exposure for both patients and staff, along with hours of wearing heavy lead protective garments. Soft tissue also cannot be visualized with the level of detail provided by MRI, which is considered the gold standard for assessing cardiac structure and function.
This MRI-guided approach changes all of that. Because the entire procedure is performed inside an MRI scanner, the operator has a live, high-resolution view of the heart's chambers, valves, and surrounding structures. At the same time, patients, operators, and staff are not exposed to ionizing radiation.
Bilchick points to the image quality as a key reason to adopt this approach. "MRI offers the best visualization of tissue," he notes. “Everything is crisp. You can see the borders of every chamber very clearly."
The procedures were performed in an existing clinical MRI scanner, not a purpose-built EP suite. Upgrades included waveguides, additional monitors, and a communication system between the control room and the scanner. Bilchick notes that this setup demonstrates that the procedure does not require a hyperspecialized facility.
A new clinical privilege for MRI-guided procedures was also created at UVA Health as a result of this work.
Treating Atrial Flutter and Watching It Stop
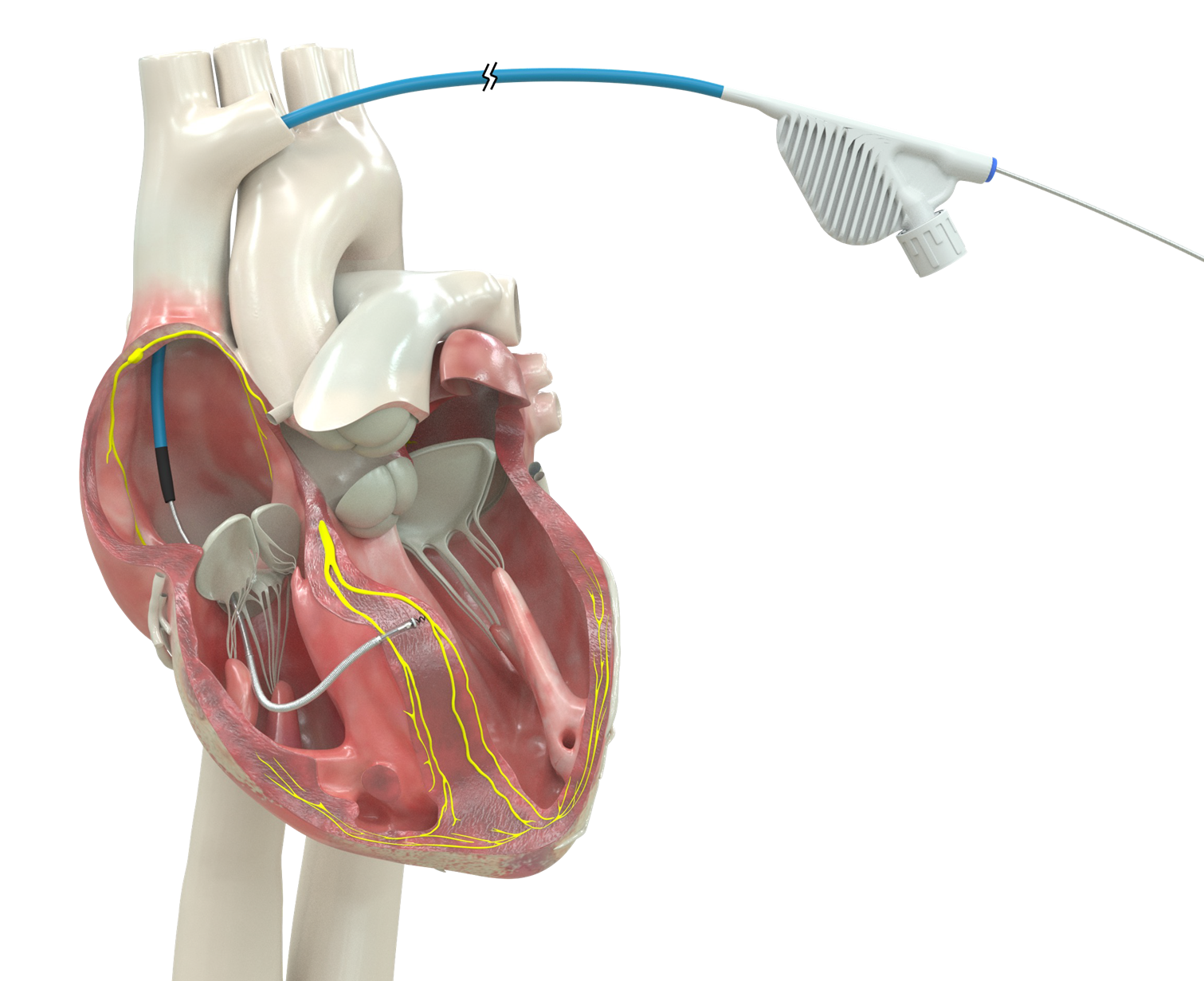
In the MRI scanner, operators directly visualize catheter movement in real time. They can track ablation lesions as they are placed and confirm electrical block across the areas of conduction.
With MRI guidance, the typical workflow includes time for anesthesia induction, vascular access, and MRI mapping followed by approximately one hour for the ablation itself.
Two of UVA’s initial three patients were still in atrial flutter at the start of their procedure. “In each case, once we reached the critical region, we watched the rhythm convert in real time from atrial flutter to normal sinus rhythm,” describes Bilchick. Clear visualization of these electrical signals despite the magnetic fields in the scanner is an impressive accomplishment resulting from many years of technology development. All patients recovered well after the procedure and were discharged the same day.
The Bigger Picture: Ventricular Tachycardia and Beyond
Atrial flutter is just the starting point. Bilchick foresees MRI-guided ablation as a game changer for ventricular tachycardia (VT), which often arises from scar tissue left behind after a myocardial infarction. "Catheter ablation for that one can be lifesaving. It can keep people from getting shocks from defibrillators or passing out or dying," he explains.
The value of MRI for VT ablation is especially strong because MRI is the gold standard for visualizing myocardial scar. In a conventional EP lab, scar boundaries must be inferred. In the MRI scanner, scar appears as bright white against a dark background. Operators can target the precise area, and repeat imaging after ablation can document how tissue properties have changed.
Bilchick also highlights potential applications beyond ablation. MRI guidance could improve cardiac catheterizations in pediatric patients with congenital heart disease, where both structural and hemodynamic data are needed at the same time, and it could also be great for obtaining targeted heart biopsies in heart failure. "I think over the next three, four years, we could see expansion of this approach at UVA to other applications," says Bilchick.
A Team Effort Led to MRI Ablation Success
Making this happen at UVA Health required more than clinical expertise. It took coordination across multiple departments, EP lab nursing and management, anesthesiology, the MRI department, clinical research coordinators, and the research MRI operations team.
“What really made this successful at UVA Health was the enthusiasm and support from all the stakeholders,” says Bilchick.
An Engineering Paradigm Shift
The engineering challenges behind MRI-guided ablation are substantial because catheter systems contain metallic components and must function safely within strong magnetic fields. MRI depends on strong static and gradient magnetic fields. Recording clean electrograms inside a magnet, while delivering ablation energy and staying within safety limits for tissue heating, required years of bioengineering development.
For Bilchick, the achievement is hard to overstate. “This represents an incredible achievement in catheter engineering, ECG technology, and procedural mapping. I would describe it as a paradigm shift in the treatment of arrhythmias, and the technology could ultimately extend to many other interventional cardiology procedures in the coming years.”