Considering Tuberculosis in Pediatric Septic Arthritis
A hacked cough into a tissue with droplets of blood is an image so ingrained in our cultural imagination that it’s easy to mistake it for the sole presentation of tuberculosis. Especially in the United States, where TB remains relatively rare.
But following 2020, cases have been swinging upwards. The pandemic’s supply chain disruptions only accelerated TB’s drug resistance, as many people were unable to get their medications. And when they got finally got their once life-saving prescription, they found that it no longer worked.
In the United States, TB cases rose to a little over 10,000 in 2024. As a result, many doctors are now seeing TB for the first time in their careers. A deeper understanding of the many ways in which TB can present can improve diagnosis.
Leigh Lather, MD, and Keith Bachmann, MD, pediatric orthopedists at UVA Health Children’s, share what drove their diagnostic decision-making when a young boy came into the emergency room for knee pain. Ultimately, he was diagnosed and treated for tuberculosis.
Unusual Presentation
For over 3 years, this young boy had struggled with swelling and pain in his right knee. His mom confirmed that he had a persistent limp. When they went to the doctor to be seen for it, the boy’s skin test was positive for TB. His family was advised to take him to the UVA Health Children’s pediatric emergency department.
He had a known TB exposure and was from a country where TB was endemic. But most of the other symptoms doctors might associate with TB, like fever, night sweats, persistent cough, or weight loss, were not present.
A Wide Differential
The explanations for a child with recurring knee pain are nearly endless. The most dangerous of these, a septic bacterial infection, needed to be ruled out quickly. But other causes for recurrent joint swelling and pain over 3 years include everything from parasite-borne pathogens like Lyme disease, rheumatologic conditions like lupus or juvenile idiopathic arthritis, and even hematologic malignancies like hemophilia. Statistically, in the United States, even rare bone cancers like osteosarcoma are more common than a case of TB presenting as knee pain in the absence of all other symptoms.
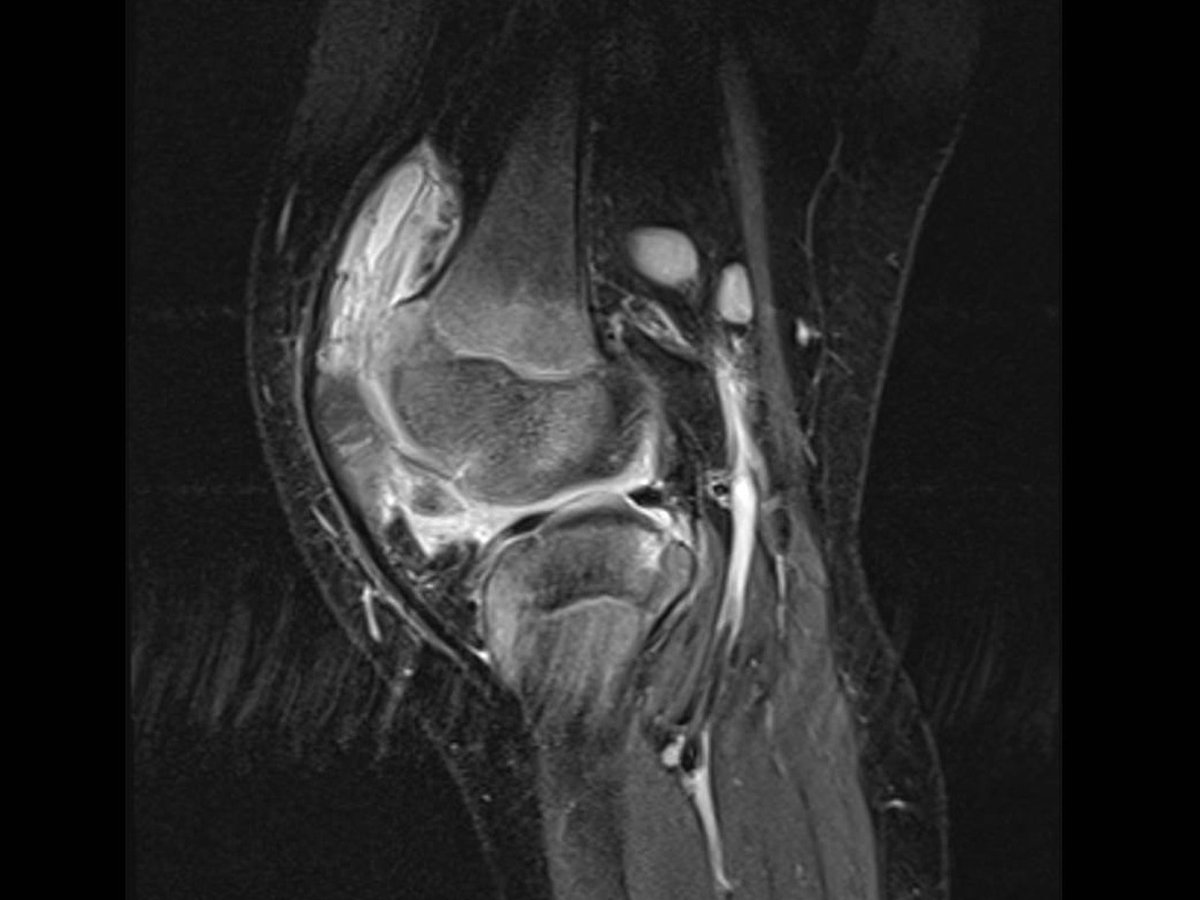
To begin to narrow the list, the team started with imaging. And on MRI, an unexplained effusion was seen. “When there’s effusion without other cause, an aspiration is performed to determine the cause. Based on the cell count from the aspiration, we proceeded with arthrotomy,” Bachmann says.
The tissue sample collected during arthrotomy revealed synovial tissue with mycobacterial-associated necrotizing granulomatous inflammation. “It was an abnormal picture, but we did not know the synovial tissue had mycobacterial-associated granulomatous inflammation until pathology evaluation was performed, so we were not sure we were looking at TB. But we suspected it was not an aerobic or anaerobic bacterial septic arthritis,” Bachmann says.
Pathology’s Pivotal Role
It was only after pathology tested the tissue that the team could confirm that the patient’s arthritis was caused by TB.
Bachmann shares, “The key for diagnosis in this case was the pathology. From an orthopedic standpoint we have an adage that you culture everything you biopsy and you biopsy everything you culture.”
Just like that, a wide differential was slimmed to 1 treatable cause.
Keeping TB on the Table
There was a completely clear chest x-ray. A lack of standard systemic symptoms. But every reason to keep TB on the diagnostic table until it was cleared.
Lather adds that TB “Should be considered in anyone with insidious (slow) onset of septic arthritis that does not respond to standard antibiotic treatment, particularly if they are from an endemic area.”
Extrapulmonary TB can occur in almost any area of the body and befuddle diagnosticians from any specialty. Blood in the urine, headaches, hoarseness, skin nodules, and back pain are just some of the atypical ways that TB has presented. Understanding what makes a patient at risk for TB and the importance of pathology are crucial as cases continue to grow.
A Happy Outcome
An infectious disease specialist followed up and started the child on a four-drug cocktail that is standard for TB for 9 weeks.
At the end of those 9 weeks, the young boy could straighten his knee, run around, and wasn’t experiencing pain or limping. For the child, this was life changing: after years of being told there was nothing to be done for his pain, he was finally able to be a child again.
Bachmann shares: “He has not had any other issues from his knee now that it has been treated, but the risk of arthritis at an earlier age is elevated.”
After this child’s diagnosis, the Virginia Department of Health also conducted contact tracing that led to others in his family being diagnosed and treated.